Embedded Files
Incidence of road injuries in Argentina
[Download detailed results tables: Click Here
Report in Spanish (Long Version): Click Here]
Last Updated: Apr 14 2011
Important: Please note that the results presented here are preliminary. Additional adjustments will be necessary as the results are made consistent with the ongoing Global Burden of Disease (GBD-2005) project, for which the results presented here are an input. Final estimates of the GBD-2005 study will be released in late 2010.
About this report
About this report
Reliable statistics of road injuries are an essential input for describing the public health burden of injuries, evaluating the impact of safety policies, and benchmarking achievements. While injury surveillance systems are common in high income countries, most low and middle income countries are unlikely to have such capacity for several decades. In the interim, estimates should be derived by harmonizing injury statistics from the wide array of data sources that may be available in a country or region.
This report summarizes our findings for the incidence of deaths and non-fatal injuries from road crashes in Argentina. It is one of a series of national road injury assessments that we are producing during the course of this project. The intended audience of these reports includes the global donor community, the international research community, and national health and transport policy makers. We are committed to keeping this project open-source and collaborative in nature. All readers are encouraged to provide feedback to help improve methods, incorporate other sources of information, and suggest more effective methods for communicating these results.
Summary Results
Contents

In 2005, road crashes resulted in 5,093 deaths in Argentina representing an annual injury rate of 13.6 deaths per 100,000 people (Figure 1). The road injury death rate of Argentina was 2.3 times the death rate in countries with the best road safety performance (Sweden, UK, and Netherlands).

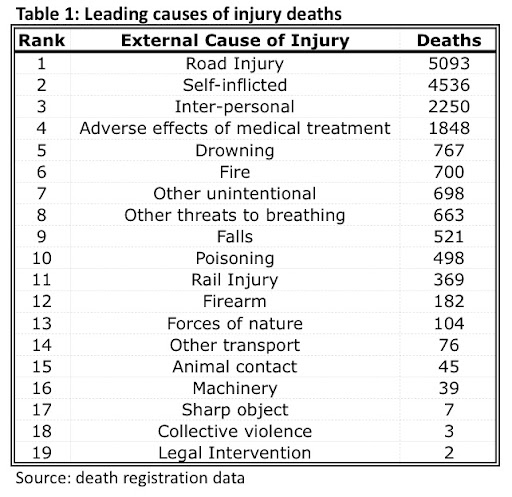
Injuries as a whole, including from unintentional and intentional causes, resulted in 18,548 deaths or 6.3% of all deaths in Argentina in 2005. Road injuries are the leading cause of injury deaths in Argentina, resulting in more deaths than suicides, and more than twice the number of homicides (Table 1). In 2005, road injuries accounted for 28% of all injury deaths in Argentina.
How did we compute these estimates?
How did we compute these estimates?
Our general methodology for estimating deaths and non-fatal injuries involves piecing together data from a wide array of sources that typically include death registers, hospital records, funeral records, health surveys, and police reports. This requires filling information gaps, mapping from varying case definitions, deriving population based incidence estimates from sources that may not track denominator populations, and appropriately reapportioning cases assigned to poorly specified causes. For a general description of the broad methodology, please visit the Methods-overview section of our website.
The following sections describe the specific data sources used, the estimation methods, and the key results for our estimates of road injuries in Argentina. The analytical adjustments to the data introduce uncertainty in the estimates. Thus, wherever possible, we have outlined the effects of the adjustments on the estimates.
Overview of data sources
Overview of data sources
We estimated the incidence and distribution of road injury deaths in Argentina using national death registration data obtained from the WHO Mortality Database. We estimated the distribution of non-fatal injuries using the national hospital discharge records.
Estimates of road injury deaths
Estimates of road injury deaths
Our review of data sources for estimating national road injury deaths in Argentina revealed two primary data systems: national death registration data and the national register of traffic records, which is maintained by the national road safety agency, RENAT). n this study, we have computed estimates of national road injury deaths from the former (death registration) and compared them with those reported by RENAT. We obtained death registration data from the publicly available WHO Mortality Database. These data are tabulations of deaths recorded by national civil registration systems. Typically these systems record age, sex, and causes of death coded using principles of the International Statistical Classification of Diseases (ICD). We only analyzed death registration data from 1980 to 2007, which had causes of death coded to ICD-10 categories.
Reclassification to GBD-2005 definitions: We reclassified age into 38 age-sex groups. The age definitions match those used by the GBD-2005 project and are available on the GBD-Injury expert group website. Click here to go directly to the age definitions.
We reclassified the ICD coded deaths to the definitions of road injuries (and other injuries) as recommended by the GBD-Injury expert group [Click here for full details]. These definitions map all ICD codes for external causes of injury to 48 fully-specified cause categories and 21 partially-specified and undetermined cause categories. The fully-specified cause categories include nine road-user categories:
Pedestrian (V01-V04, V06, V09),
Bicyclist (V10-V19),
Two-wheeler rider (V20-V29),
Three-wheeler occupant (V30-V39),
Car occupant (V40-V49),
Van occupant (V50-V59),
Truck occupant (V60-V69),
Bus occupant (V70-V79), and,
Other road injury (V80, V82, V83, V84, V85).
In addition, there are two partially-specified sub-categories of road injuries:
Road injury - unspecified occupant, i.e. not pedestrian or bicyclist (V87-V88), and,
Road injury - unspecified road user (V89, Y85.0)
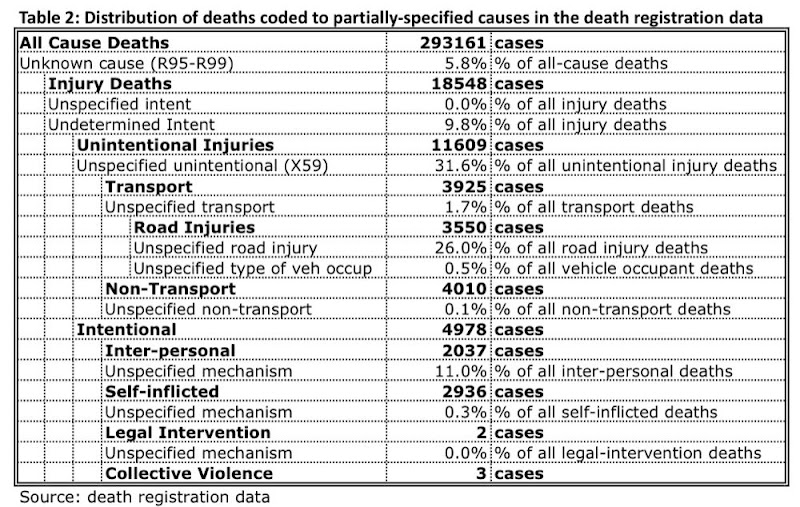
Table 2 shows the distribution of the 18,548 injury deaths reported in the death registration data for the year 2005. It should be noted that the 21 partially-specified categories have a hierarchical structure of specificity and many of these categories are not related with road injuries.
We assessed the quality of the death registration data based on the distribution of the number of deaths in the partially specified categories. As shown in Table 2, the quality of the death registration as measured by the fraction of death registration cases assigned to partially specified categories has two key problems. First, 31.6% of all deaths coded to unintentional injuries do not specify a mechanism for the injury. Further, over one-fourth (26%) of deaths assigned to road injuries do not have a road-user specified. The first introduces uncertainty in the estimate of total road injury deaths, and the second in estimates of the incidence of road injuries disaggregated by road-user.
Reallocation of injury deaths coded to partially-specified causes:
The deaths classified to partially-specified and undetermined cause categories were redistributed over the fully-specified categories. All redistributions were done in proportion to the number of cases in the fully-specified causes within age-sex groups. The redistribution is done in 21 steps, one for each partially-specified category. This respects the information content in the hierarchical structure of the partially-specified categories. Thus, several of these steps do not affect the road injury estimates. For instance, the category of firearm: undetermined intent was redistributed over the categories for firearm: unintentional, firearm: self-inflicted, and firearm: inter-personal. This redistribution step has no effect on the road injury estimates. Only the redistribution of the following partially-specified categories has an effect on road injury estimates: Road injury - unspecified occupant, i.e. not pedestrian or bicyclist,
Road injury - unspecified road user,
Unspecified transport injury,
Unspecified unintentional injury,
Unspecified mechanism - undetermined intent,
Unspecified mechanism - unspecified intent,

The effect of these redistribution steps is evident in Figure 2, which shows the change in the estimated number of road deaths after each redistribution step. The death registration data has 3,550 deaths specified as road injuries . As expected from the distribution of deaths shown in Table 2, there is a substantial increase in the estimates of road injury deaths during the redistribution of deaths coded to partially specified causes. This occurs when deaths coded to unintentional injuries- unspecified mechanism are reallocated. This results in an increase of about 40% in the road injury deaths.
Adjustments that have not applied yet: Two key adjustments that are likely to modify the road injury death counts have not been applied yet. First, we have not reallocated deaths coded to unspecified causes outside the ICD injury chapter. This reallocation has not been done yet because research into the causes of deaths coded to this category is currently ongoing. However, it should be noted that in Argentina, only a relatively small fraction (5.8%) of deaths are coded to this category and the effect on road injury death counts is thus expected to be small.
Second, we have made no adjustments to account for incomplete death registration because estimates of completeness of global death registration data are currently being developed. However, our preliminary comparison of total all-cause deaths reported in the death registration data analyzed by us with deaths reported by the UN Population Division suggests that death registration in Argentina is near complete. It should be noted that both of these adjustments would increase the estimated death counts. Thus, the mortality results presented here likely underestimate the true number of road injury deaths.
Comparison of our estimates with other sources
Comparison of our estimates with other sources
Our estimate of road injury deaths (Figure 3) in Argentina are 45% higher than those reported by official government statistics in the 2009 WHO Global Status Report on Road Safety. The official government statistics in the WHO report are based on national health data from the Ministry of Health. While the details of the methods used by the Ministry of Health for the official estimates are not clear, Figure 3 suggests that the numbers are nearly identical to the police/RENAT data. However, our analysis of the death registration data shows that the police data substantially under-report road traffic deaths in Argentina.
Road deaths by age and sex
Road deaths by age and sex

Most road deaths in Argentina occur among adult males (Figure 4a). Over 3/4th (77.2%) of all road injury deaths were men and over 3/4th of these men (75.3%) were adults older than 20 years. Death rates (Figure 4b) among men are 3.5 times those among women overall. Men have higher death rates for all age groups but the gender differential is smaller among the elderly. Both death counts and death rates rise dramatically in the transition in age from childhood to young adults. Death rates continue to rise with age and are highest among the elderly.
Such age and sex patterns in deaths and death rates are consistent with those seen in other countries. For the most part, the gender differentials in death rate are a result of higher exposure to road traffic among men in combination with higher risk-taking behavior. Similarly, the age pattern of death rates partly reflects patterns of exposure and partly case-fatality rates. While exposure to road traffic declines with age among older populations, the bio-mechanical tolerance to injury (i.e. the likelihood of death in the event of a crash) also declines, resulting in increasing death rates with age.
Road deaths and non-fatal road injuries by road-user type
Road deaths and non-fatal road injuries by road-user type


More than half (55%) of all deaths from traffic crashes in Argentina in 2005 occurred among car occupants (Figure 5). Pedestrians and motorized two-wheeler riders, result in an additional 17% and 11% of road traffic deaths, respectively. Although motorcyclists comprise only 11% of road traffic deaths, they comprise a much larger fraction of severe non-fatal injuries. Figure 6 shows the distribution of road-traffic related hospital discharges in Argentina. Motorcyclists comprised 30% of hospital discharges, ahead of vehicle occupants.

Thus the burden of motorcycle crashes is underestimated in mortality data. The large burden of injuries among motorcyclists in Argentina is of special concern. Motorcycles are among the most risky modes of transport. It is already well known that in South-East Asia motorcycles comprise a large proportion of the vehicle fleet and this is reflected in their road injury statistics. However, our analysis suggests that motorcycle fleets and the injuries resulting from their use are rapidly rising in parts of Latin America as well.
Acknowledgements
Acknowledgements
These country reports were produced as part of a project funded by the World Bank Global Road Safety Facility. The results presented here are based on secondary data analysis of data collected by various national and international agencies. The analysis presented in this report was lead by Dr Clotilde Ubeda, Instituto Nacional de Epidemiología “Dr. J.H.Jara” (INE), Administración Nacional de Laboratorios e Institutos de Salud (ANLIS) Malbran Argentina. The following scientists made substantive contributions to the work: Victoria Espitia-Hardeman, Nagesh N. Borse, Ann Dellinger, Daniel Ferrante, Raquel Peltzer, Kavi Bhalla, and Jerry Abraham. In addition, Dr. Bruno Linetzky provided valuable guidance to the analysis. Dr Ubeda conducted this research as part of a research fellowship funded by the Road Traffic Injury Research Network. She was hosted by the US Centers for Disease Control, Atlanta, Georgia.

Page updated
Report abuse